The UK National Screening Committee (NSC) has reached its decision on screening and the answer was largely that they don’t recommend it. Even for those at the highest risk. Black men over 45 who have twice the risk of white men and men over 45 with a family history who are at 2.5 times the risk of other men.
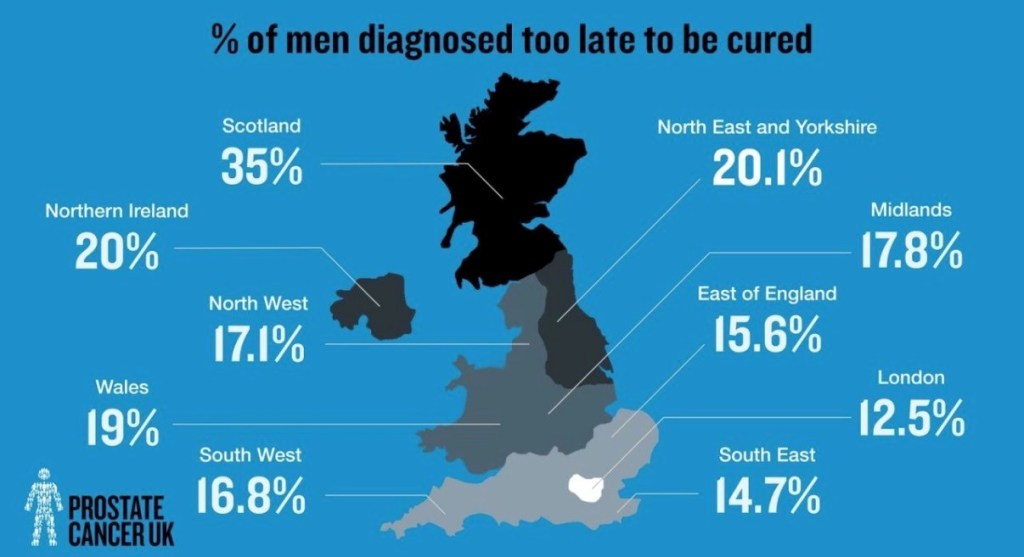
The numbers are scary! In some areas of the UK, 35% of men are terminal at diagnosis, like I was, and the national average is around 17% of men or, in numbers, that’s around 10,000 men, every single year! 12,000 men die every year that’s one every 45 minutes. Remember these numbers but I will come back to them.
The treatment for advanced stage prostate cancer is absolutely life changing, affecting every single aspect of life adversely. Although we prefer to use hormone deprivation as terminology, the reality is that it’s chemical castration. Let that sink in for a bit, chemical castration! Removal of male hormone, testosterone that men need to power their drive, including sex drive, muscle growth, bone health, erections, masculinity. Removal of it is complete emasculation. You lose muscle mass, ability to gain erections, libido, bone density, body hair and you gain weight and hot flushes. It’s great being a menopausal man, honest! The added bonus of course is that you’re also going to die prematurely as well. I wrote about this in this article https://runningintocancer.co.uk/2026/01/22/the-hits-and-misses-of-living-with-stage-4-prostate-cancer-and-a-few-of-the-things-you-gained-but-wished-you-hadnt/
Caught early, prostate cancer is generally curable but usually asymptomatic. However, we don’t have a screening programme to catch it early. Instead we rely on opportunistic testing which is where men hear the stories of the likes of myself and Sir Chris Hoy and pluck up the courage to ask their GP for a simple PSA blood test and even then there are many GP’s who flatly refuse men a test which is not what their guidelines require them to do.
Historically, men who had a high PSA reading went on to have a biopsy that was done trans rectally with a risk of sepsis and men with cancers that were never going to cause them harm had radical treatment, such as removal of the prostate or radiotherapy, that could lead to significant side effects like impotence and/or incontinence.
That pathway is now a thing of the past and treatments have improved massively with prostate removal (prostatectomy) now done by robot and radiotherapy is much more targeted. In addition, biopsies aren’t done before a multi parametric MRI scan which means they are better targeted and also done trans perennially thus reducing risk of infection (sepsis).
There’s no doubt in anyone’s minds that the harm of overtreatment is massively reduced compared to 15-25 years ago and yet the NSC continue to insist that the risk of overtreatment harm outweighs the harm of late diagnosis, including premature death!
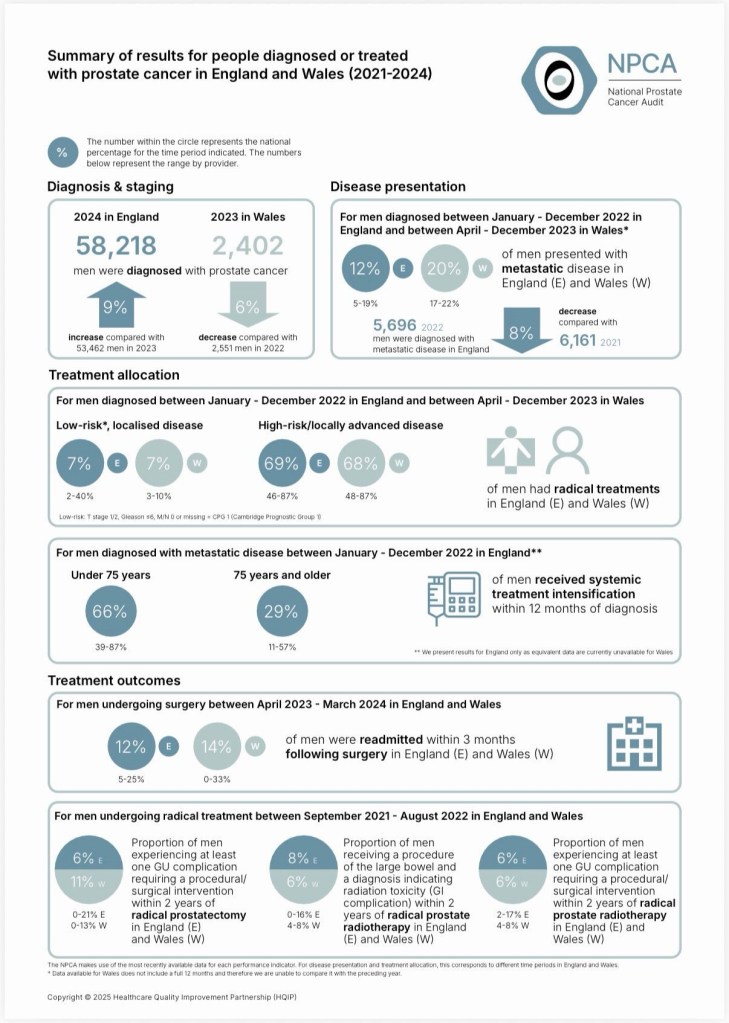
Let’s look at the numbers then. The National Prostate Cancer Audit (NPCA) showed that 7% of men with low grade cancer, that was never likely to cause them a problem, went on to have radical treatment. That is less than 400 men!
69% of men with high risk locally advanced prostate cancer went on to have radical treatment that’s c. 12,300 men.
Just over 1,000 men had an emergency readmission within 60 days of surgery.
Just under 400 men (6%) required a procedural/surgical intervention within two years of prostatectomy. Approx. 1,000 men (8%) had radiation toxicity requiring intervention within 2 years whilst that was c. 750 men (6%) for men who had a prostatectomy.
It’s a possibility that some of those men with high risk locally advanced prostate cancer may not have needed radical treatment and that’s clearly a gap in the knowledge of health care professionals that needs addressing but, even if they all did need radical treatment, it’s barely more than 2,000 men requiring subsequent interventions (therefore potentially harmed) and only 400 men with low grade cancer had radical treatment, which is a big improvement over the last decade.
Now let’s go back to the numbers for late stage diagnosis. 10,000 men diagnosed at stage 4, incurable, call it terminal if you like. 12,000 deaths every year, one every 45 minutes.
Every single one of those 10,000 men diagnosed de novo stage 4 having every single aspect of their lives adversely affected and knowing that they’ll die of their cancer unless something else gets them first.
The NPCA also said that only 66% of men under 75 received systemic treatment intensification (best Standard of Care) within 12 months of diagnosis. That’s real harm! Substandard treatment for metastatic disease.
Now please tell me what causes most harm!
For anyone wanting a deeper dive into the NPCA State of The Nation Report here’s the link https://www.natcan.org.uk/wp-content/uploads/2025/10/NPCA-SotN-2025.pdf
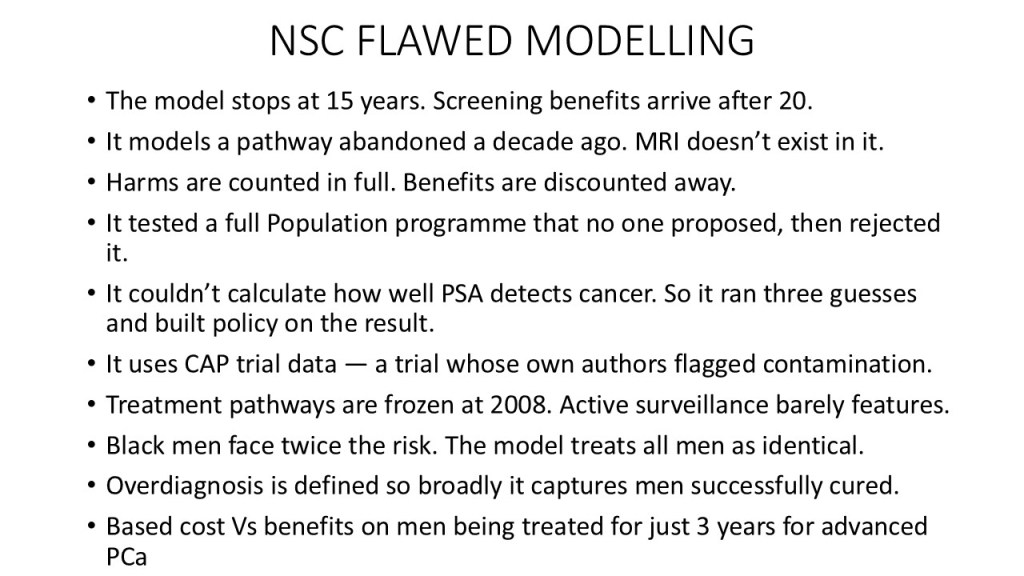
I spent a fair amount of time responding to the NSC’s consultation process, including a day preparing my detailed response, along with another 900 members of the public. All of us completely ignored just proving what a pointless exercise it was. I also went through the NSC summary reports and read in detail the consultation response from Prostate Cancer Research (PCR). I was, on behalf of Tackle Prostate Cancer one of the 18 co-signatories to PCR’s response to the NSC. It’s fair to say that the modelling used by the NSC was seriously flawed and used out of date data and diagnostic processes. I summarised some of the flaws in this slide from a recent presentation I gave recently to Worcestershire Prostate Cancer Support Group:-
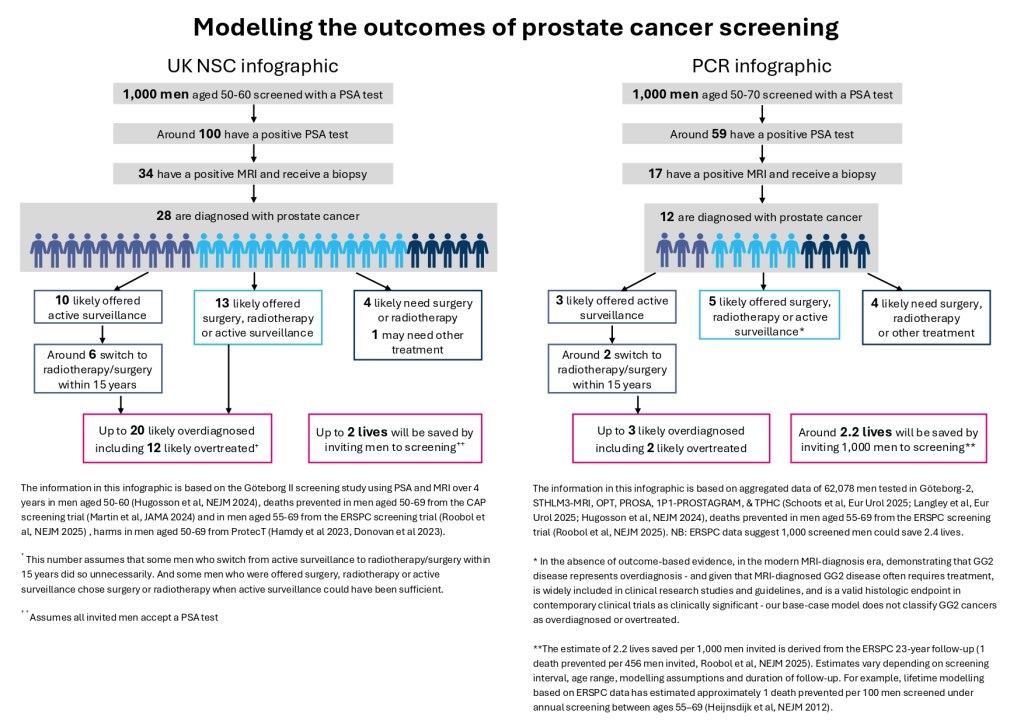
PCR commissioned their own review of the NSC data and the comparison between the outcomes shown in the NSC report and that in PCR’s is really stark as per this infographic below used with permission.
This is a link to PCR’s page regarding the NSC consultation https://www.prostate-cancer-research.org.uk/uk-nsc-decision-falls-short-of-targeted-screening-recommendation/
Where are we now?
The NSC recommendation will now be considered by the health ministers of the different UK countries who will ultimately decide on the future direction. It seems highly unlikely that they’ll do anything other than accept the recommendations especially given that government and Prostate Cancer UK are funding the TRANSFORM trial. We could hope for a request from ministers to re-model the outcomes using more informed, up to date, data but that would take a while. I don’t think it will happen in any event so that leaves us with zero progress on screening since my diagnosis 9 years ago!
What are we left with?
Basically, awareness raising to ensure that men get tested opportunistically by their GP. This is seriously flawed though as a) it requires men to know that they have to ask for a test and; b) it exacerbates the already huge health inequalities that see people from poorer socioeconomic backgrounds fare less well in health terms and; c) it requires GP’s to follow their guidelines on testing asymptomatic men and, regrettably, lot’s of GP’s are still living in the dark ages as far as PSA testing is concerned and spout the argument that “testing does more harm than good” when, in the reality they are completely out of date on the modern diagnostic pathway.
At the very least we need government to issue much stronger guidelines to GP’s encouraging them to proactively engage with asymptomatic men in the high risk groups (current guidelines discourage them from doing so). There also needs to be much better GP training on the harms of late diagnosis of prostate cancer.
I’m now going to touch briefly on the TRANSFORM trial and this is my opinion and not that of any charity I’m involved with. The trial is the biggest screening trial, costing £42m, ever conducted and it has now started recruiting. We are told that there’ll be an interim report after two years and that the NSC have agreed to consider the evidence produced. However, there is no certainty that, after two years, any evidence would meet the requirements of the NSC. What if it takes 10 years to produce evidence that would satisfy the NSC and then maybe another 5 years to set up a screening programme? In that 15 years another 180,000 lives will have been lost, many of which could have been prevented. As my friend Professor Alison Birtle said in her Radio 5 interview with Tony Livesey on 28.05.26 at 10:16pm “We simply can’t wait, I’m fed up of going to my patients funerals”. I’m afraid that the TRANSFORM trial made it much easier for the NSC to recommend against screening and instead to wait. Now is not the time to be doing nothing!
I’ll leave you with a final thought. If you heard the so called “experts” on TV and radio saying that screening does more harm than good, are you then going to ask your GP for an opportunistic PSA test?
For goodness sake let’s change the narrative. It’s like a stuck record and is stopping lives being saved!
The views in this article are mine and not necessarily the views of any charities I am involved with.

Absolutely spot on Tony, this feels like one of those horrible nightmares where you are trapped and no matter how much you shout, nobody is listening. Throuble is you wake up from those!
LikeLike
Spot on Tony. This feels like one of those nightmares where you are trapped and no matter how much you shout, nobody is listening, only difference is you wake up from those!
LikeLike
Your summary is spot on Tony, well done.
LikeLike